Indigenous peoples mostly live in urban centers rather than reservations and are a heterogeneous group representing hundreds of nations, each with their own cultural practices and history. Individuals have different preferences for the term used to describe Indigenous people in the U.S., including American Indian, Native American, or by the names they call themselves in their own languages. The main groups of Indigenous people residing in Minnesota are the Dakota and the Chippewa, also referred to as Ojibwe or Anishinaabe. This resource uses the term “American Indian” to refer to Indigenous people of North America and Minnesota. In certain instances, the term “American Indian” in conjunction with Alaskan Natives is used as that is the term used in some state laws and the U.S. Census for Indigenous people. It’s important to ask about individual preferences. View: The Impact of Words and Tips for Using Appropriate Terminology from the National Museum of the American Indian.
NOTE: Understanding the role culture plays in health care is essential. Still, patients are individuals – each person’s preferences, practices, and health outcomes are shaped by many factors, a concept known as intersectionality.
 American Indians in Minnesota
American Indians in Minnesota
There are nearly 163,000 American Indian Minnesotans and about 5.2 million in the U.S., making up about 2% of the population. The Phillips neighborhood of Minneapolis has the third largest urban American Indian population in the U.S.
Learn more:
- American Indians, Indian Tribes, and State Government
- Partnership to Advance Tribal Health (PATH)
- Comagine Health PATH
- Indian Health Service Fact Sheets (IHS is a U.S. federal government health care entity on many reservations, outlined as a provision in treaties.)
- Optimizing Rural Health Assets
Nearly all American Indians speak English as their primary language. The most common American Indian language spoken in Minnesota is Ojibwa. Fewer than 10% of American Indian Minnesotans say they speak American Indian languages at home and only a fraction of these speakers say they speak English “less than very well.”
- Interpreter Roster: Spoken Language, Health Care, Minnesota Department of Health
- Resources for better Patient-Provider Communication
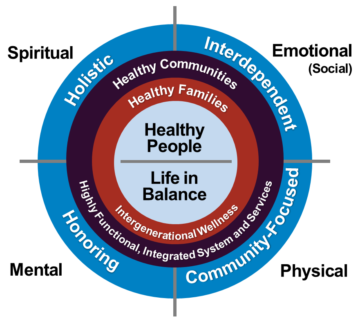
American Indian Holistic Approach to Health
American Indians in Minnesota experience worse social and health outcomes than any other population. Some health issues are biologically tied to race, but many are tied to social inequities, including poverty. Health conditions experienced by American Indians include high rates of heart disease, cancer, diabetes, alcohol-induced illnesses (e.g., chronic liver disease and cirrhosis), influenza and pneumonia, drug-induced illnesses, kidney disease, mental illness, and Alzheimer’s and other dementia.
- The premature death rate for American Indians in Minnesota is more than three times higher than the rate for whites.
- Within Minnesota alone, the rate of type 2 diabetes is 600% higher than for whites.
- About 26% of American Indians in Minnesota experience optimal diabetes care, compared with 46% of Whites.
- Adult American Indians in Minnesota (43.7%) have the highest rate of obesity, compared to Hispanics (35.9%), Blacks (36.7%), or Whites (33.6%).
- 55% of American Indians age 50+ in Minnesota are up to date with colon screening compared with 73% for Whites.
- The rate of heart disease among American Indians has doubled in the last 50 years and is now the for those in Minnesota.
- Cancer is the for American Indians in Minnesota, who are 33% more likely to develop cancer and 78% more likely to die from cancer than whites.
- 24% of Ojibwe in Minnesota ages 45-64 have one or more disabilities, compared to 12% for the overall population.
More data on disparities in health and health care for American Indians - The Health and Well-Being of Minnesota’s Adolescents of Color and American Indians
- Memory Keepers Medical Discovery Team
- Indian Health Service: Disparities
- CDC: Chronic Diseases
Health Check: How do American Indians compare to your overall patient population across process and health outcome measures? It’s important to note that American Indians are twice as likely to be diagnosed with diabetes, have a greater prevalence of obesity, and are more likely to be smokers than other populations.
Minnesota Clinical Quality Measures 2017 | |||||||
Optimal diabetes care | Optional vascular care | Adolescent mental health screening | Pediatric oversight counseling | Optional asthma control-A | Optional asthma control-B | Colorectal cancer screening | |
| American Indian | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| White | ↑ | ↑ | ↑ | ↑ | ↑ | ↑ | ↑ |
| ↑ = Above average, ↓= Below average, Blank = Similar to average | |||||||
Social determinants of health, sometimes also referred to as social drivers of health (SDOH), are economic and social conditions that influence the health of people and communities. American Indians often experience race or ethnicity discrimination, which may impact housing, employment, legal status, and likelihood of experiencing violence and bullying. Dealing with discrimination is associated with higher reported stress and poorer reported health.
- 31.3%of American Indians in Minnesota are below the federal poverty level, compared to 8.2% of Whites. About 37.1% of American Indian children live in poverty.
- The median income for American Indian families (regardless of family size) in Minnesota is $36,900, compared to $67,000 for White families.
- The teen birth rate for American Indians in Minnesota is 57.8 per 1,000 births, compared to 10.1 for Whites. Teen birth rate is a key indicator for future poverty, low educational achievement, and poor health.
- American Indians make up 13% of homeless adults in Minnesota, but only 1% of the population.
- American Indian children in Minnesota are five times more likely to be reported as victims of abuse than white children, and 10 times more likely to end up in foster care.
Learn more:
Minnesota has 11 federally recognized Indian tribes, each with reservation land: Four Dakota and seven Ojibwe. Although requirements differ, enrolled membership is based on each tribe’s constitution. Many aspects of American Indian culture today reflect the assimilated culture of the general U.S. population. Generational differences impact social practices.
The American Indian concept of family includes immediate and extended family members, as well as community and tribal members who may not be biologically related. American Indians have a tradition of respect for elders. Many tribal communities have a custom of showing respect for elders by allowing them to speak first without interrupting and giving time for opinions and thoughts to be expressed. It is disrespectful to openly argue or disagree with an elder. It is customary for elders to eat first at home and during community events, often being served a plate at their seat.
American Indians have some cultural practices of smoke, including smoking ceremonial tobacco and smudging. Tobacco, asemaa in Ojibwe, is smoked in ceremonial pipes.Smudging is burning small amounts of traditional medicine like sage, and wafting the smoke over a person, or just letting the smoke drift, as a way of purifying, cleansing or praying. American Indians have the highest cigarette or commercial smoking rates of all U.S. racial and ethnic groups, which may be related tobacco traditions passed down for generations. Today, the cigarette smoking rate for American Indians is 21.9% —four times that of the general population. Many are working to restore traditional tobacco practices, which includes using traditional/ceremonial tobacco and reduce commercial tobacco abuse like cigarette smoking.
Forced assimilation and repeated unfulfilled agreements in treaties with American Indians, such as the 1787 agreement with tribes to provide American Indians with free health care on reservations, has resulted in a lack of trust of the majority culture and state, local, and federal government.
Learn more:
The traditional American Indian diet is hyperlocal and seasonal and very healthy with no processed foods, no sugar, no wheat (or gluten), no dairy, and no high-cholesterol animal products. It’s naturally low glycemic, high protein, low salt, and plant-based with lots of grants, seeds, and nuts. As European settlers spread across America and displaced Native American tribes, however, Native food customs were completely disrupted.
Unfortunately, due to a variety of SDOH factors, and historical factors such as reservation rations (e.g., lard, flour, and more), many American Indians now consume a diet of low nutritional value and processed foods. This way of eating contributes to obesity, heart disease, and other health conditions. Contrary to popular belief, fry bread is not a traditional food. Created from the reservation rations provided via the U.S. government, fry bread was created as a means of survival and has become a staple food in many Native American households. In Minnesota, native advocates and health experts are promoting a return to ancestral diets. Alcohol use among American Indians is also high, contributing to the heavy carbohydrate intake and adverse health conditions.
Learn more:
- North American Traditional Indigenous Food Systems
- How Owamni Became the Best New Restaurant in the United States
Health care professionals must have an understanding of and respect for a wide spectrum of beliefs and religious preferences of American Indian patients to provide optimal care. The overarching guide is that life must be lived in balance (of mind, body, spirit and connection to the land and community) to support individual and family health and wellness. Native elders may incorporate traditional healing practices into treatment or wellness practices.
Poverty, a major SDOH, results in lack of access to healthy food and preventive health care. Low health literacy and understanding of Western medicine’s terminology may contribute to uninformed health decisions. Lack of health care trust and lack of availability of culturally appropriate or culturally sensitive health care may result in health care avoidance. The IHS, a U.S. federal government health care institution, provides a comprehensive health service delivery system for about 2.2 million of the nation’s estimated 3.7 million American Indians, so a large percentage uses health care outside of local tribal health care systems. Often, IHS institution do not have all the resources required to meet medical needs and use a referral system to other health care institutions that offer more resources and higher levels of care.
Learn more:
Genocide, abuses while forced to attend boarding/residential schools, forced relocation, banned languages, second-class legal status, limited mobility to choose where to live, substandard public education, racism, and other barriers have resulted in loss of cultural practices, and historical trauma for some American Indians, the effects of which continue today. Carried across generations, this trauma should be considered in mental health and physical treatments.
The high rates of alcohol; substance use and mental health disorders; suicide; violence; and behavior-related morbidity and mortality in American Indian and Alaska Native communities continue to be disproportionately higher than the rest of the U.S. population. These high rates result in American Indian and Alaska Native people report serious psychological distress 2.5 times more than the general population.
Learn more:
- American Indian Substance Abuse Prevention Activity in Minnesota
- Trauma-Informed Care
- Historical Trauma and Cultural Healing
- The Impact of Discrimination
- A culturally appropriate guide for empowering tribal youth and preventing suicide
Taking care of family is part of everyday life in tribal communities, with one in three American Indian adults serving as caregivers to a friend or family member with a health problem or disability. Tribal communities are resilient and strong, with values of respect and reverence for elders and community service orientation. Tribal communities also have ways of healing and caring for health through storytelling, traditional physical activities, or ceremonies that work alongside Western medicine, providing social connection and holistic healing.
The National Indian Council on Aging, Inc. (NICOA) advocates for improved comprehensive health, social services, and economic well-being for American Indian and Alaska Native elders.
Learn more:
Life expectancy for American Indians in the U.S. is 71.8 years, compared to 78.8 years for the country. American Indians in the U.S. die from heart disease, influenza and pneumonia, chronic liver disease, suicide, alcohol-related causes, and septicemia at higher rates than other Americans.
Terminally ill American Indians are less likely to receive hospice and palliative care than any other racial/ethnic group, with fewer than 1/3 receiving these services compared to over 45% of EuroAmericans. Barriers to access resulting from lack of financial resources, lack of tribally based and staffed end-of-life services, contribute to the gap.
Hospice care is a critical component of end-of-life healthcare that focuses on providing comfort, support, and dignity to individuals facing terminal illnesses. While hospice care is available to people of all backgrounds and cultures, it’s important to recognize that the unique cultural, spiritual, and social perspectives of American Indians require special attention. Meeting the hospice care needs of Native Americans involves cultural sensitivity, community involvement, and a holistic approach.
Building partnerships and seeking guidance from tribal elders and community leaders is crucial to expanding hospice care to Native American families. They can provide insights into cultural preferences, assist in bridging the gap between healthcare providers and the community, and help ensure that hospice care aligns with the values and traditions of the tribe.
Learn more:
- Meeting the Hospice Needs of Native Americans
- End-of-Life Services in Tribal Communities
- Advance Care Planning Among American Indian, Alaska Native, and Native Hawaiian Peoples
Other Populations in Minnesota
African American | American Indian | Asian Indian | Bhutanese | Cambodian | Deaf / Hard of Hearing | Ethiopian | European American | Latinx | Hmong | Iraqi | Karen | LGBTQ | Liberian | Poverty | Rural | Russian | Somali | Vietnamese