How do social determinants (or drivers) of health shape health and well-being?
Research indicates that 80% of a person’s overall health is determined by where they live, learn, work, play, worship, and age. Connecting these social determinants or social drivers to health care’s ability to influence and improve the much narrower 20% is critical to providing whole-person care and understanding. Yet, health care screening, referral, and care processes infrequently take these community-based social determinants/drivers of health (SDOH) into account. Building bridges between the community and health care holistically meets patient needs and leads to better health outcomes.
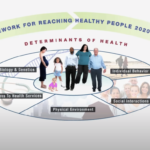
According to the CDC Healthy People 2020 project, “Social determinants of health care are conditions in the environments in which people are born, live, learn work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.” Examples of social determinants include food, housing, education, public safety, discrimination, racism, income, and literacy.
Explore the resources below:
The Basics of SDOH
The resources below will help you appreciate the fundamentals of social determinants of health and why they play such a significant role in individuals’ health status and outlook.
 Addressing Social Determinants of Health to Improve Health Equity
Addressing Social Determinants of Health to Improve Health Equity
In this podcast, Reuben Moore, president and executive officer of Minnesota Community Care, and Jennifer Lundblad, Stratis Health president and CEO discuss how addressing social determinants of health contributes to improving health equity.
 SDOH: comparing two different lives
SDOH: comparing two different lives
This short video provides a side-by-side comparison of two individuals with very different life stories and circumstances and shows how social determinants manifest themselves during our lives.
(3-minute video)
 Healthy People 2020
Healthy People 2020This short video provides examples of two individuals and how SDOH interventions can improve health outcomes. Healthy People 2020 is a United States Department of Health and Human Services program to establish 10-year plans to reduce controllable health risks encompassed in the SDOH domains.
(5-minute video)
 SDOH 101 for Healthcare
SDOH 101 for HealthcareThis article published by the National Academy of Medicine describes how SDOH relates to health care and is an excellent “SDOH 101” reading to ground yourself in the topic.
(6-page article)
This CDC web page provides a brief overview of SDOH and includes links to explore the components and domains of SDOH. (Website)
The Agency for Healthcare Research and Quality has compiled both basic information on SDOH and in-depth looks at SDOH & Health Systems Research, SDOH & Practice Improvement, and SDOH Data & Analytics.
(Website)
Impact of COVID-19 on SDOH
COVID-19 has worsened already existing social needs gaps in our communities, states, and nationally. Our individual and population health is the combination of what our health care infrastructure and community environments produce together. We need to be aware of the ways the pandemic and long-standing injustice have affected individuals and communities by factoring SDOH into new or modified solutions and policies.
 How health equity is being affected and how SDOH screening can help
How health equity is being affected and how SDOH screening can help
This infographic from The National Institute for Health Care Management (NIHCM) Foundation communicates the interplay of COVID-19 and homelessness, which we know has increased during the pandemic and is negatively affecting health. (Infographic/website)
 Insights on racial and ethnic health inequity in the context of COVID-19
Insights on racial and ethnic health inequity in the context of COVID-19
This infographic from McKinsey & Company conveys insights on racial and ethnic health inequities in the context of COVID-19. (Infographic/PDF)
 Transforming SDOH Services in the Age of COVID-19
Transforming SDOH Services in the Age of COVID-19
This article published by Healthify underscores the strain and intensified effects the pandemic has had on our collective health. A 24-minute podcast and a video are also available. (1-page article/24-minute podcast/website)
Risk Screening Tools and Resources
The initial step to identify risk for our populations and individuals is to conduct a screening process that patients can complete independently or with assistance. Once the risk factors are clear, they can be translated into social needs, and providers can connect individuals with the most appropriate community resources. Explore a sampling (in alphabetical order) of risk screening tools and related resources.
 Accountable Health Communities Health-Related Social Needs Screening Tool
Accountable Health Communities Health-Related Social Needs Screening Tool
The Centers for Medicare & Medicaid Services’ Center for Medicare and Medicaid Innovation created the Health-Related Social Needs (HRSN) screening tool to use in the Accountable Health Communities (AHC) model. (10-page PDF)

The American Academy of Family Physicians (AAFP) EveryONE Project aims to promote diversity, address the social determinants of health, and advance health equity. Screening tools are available under Assessment and Action. (Website)
 PRAPARE Training and Resources
PRAPARE Training and Resources
The Protocol for Responding to and Assessing Patient Assets, Risk, and Experiences. (PRAPARE) was developed by the National Association of Community Health Centers (NACHC), The Association of Asian Pacific Community Health Organizations, and the Oregon Primary Care Association. (Website)
 Self-Sufficiency Outcomes Matrix
Self-Sufficiency Outcomes Matrix
The Self-Sufficiency Matrix was developed by the Center for Health Care Strategies to assesses social determinants for populations with complex needs. (2-page PDF)
E-Referral Vendor Solutions
E-referral solutions have a significant benefit as they take burden off the health care system in multiple ways. E-referral vendors provide a database of community-based organizations (CBOs) that is maintained regularly and serves as a directory of agencies that enables immediate matching from the needs-based screening to the appropriate services. These solutions can integrate with various risk-screening tools and allow CBOs to electronically receive the referral and provide feedback about how and whether a referral was acted on. A sampling (alphabetically) of several vendors is provided below; there are others in the marketplace. Each vendor has developed their product with a philosophy of how best to serve their customers and create a custom SDOH solution.
Pathways HUB Model
The Pathways HUB model is a more focused, guided, and individualized model. Care coordinators (often community health workers) work with individuals and their families over time (often three months to a year) to identify risk factors and resulting social needs, which are then translated into categories or Pathways. Pathways are followed and completed to reduce the risk factors and supported by coordinating through a central community HUB. The model is designed to be self-sustaining financially through payment for completing the Pathways. Explore the resources below to learn more about the Pathways HUB model.
 Pathways Community HUB 101
Pathways Community HUB 101This brief video from the Southwest Washington Accountable Community of Health (SWACH) gives a basic overview of the Pathways Community HUB model. (3-minute video)
 Pathways HUB Webinar w. Dr. Sarah Redding
Pathways HUB Webinar w. Dr. Sarah Redding
In this presentation, Dr. Sarah Redding, the founder of the Pathways Community HUB model, shares details, insights, and examples and provides the introductory knowledge needed for those interested in pursuing the model’s implementation in their community. (1-hour video)
 The Pathways Community HUB Institute (PCHI)
The Pathways Community HUB Institute (PCHI)
PCHI assists communities in launching HUBs and certifying that implementation meets model standards. Certification standards, like national quality metrics, enable comparisons among the national HUBs. (Website)
 Map of HUBs in the U.S
Map of HUBs in the U.SThis interactive map, created and managed by the Pathways Community HUB Institute, allows the user to see an overview of all the Pathways HUB implementations around the U.S. (Note: there are additional HUBs in development that may not be shown) (Website)
 AHRQ Pathways HUB Implementation Guide
AHRQ Pathways HUB Implementation Guide
The Agency for Healthcare Research & Quality has done extensive work and study on the Pathways HUB model and produced a guide framed around three major phases and related steps to implementing the model. (74-page PDF)
Learn about PCHI certification requirements for Pathway HUBs
This web page is a jumping-off point to understanding what is required to become a HUB, along with the steps to achieve certification through Pathways Community HUB Institute (PCHI). (Website)
 Example of a Pathway HUB in Ohio
Example of a Pathway HUB in Ohio
Learn about and explore the Central Ohio Pathways HUB. (Website)
 Example of a Pathway HUB in Michigan
Example of a Pathway HUB in Michigan
Learn about and explore the Community Connections HUB. (Website)
 Example of a Pathway HUB in Wisconsin
Example of a Pathway HUB in Wisconsin
Learn about and explore the Great Rivers HUB. (Website)
SDOH Data Analytics and Standards
The process of screening individuals for risk, making referrals, and receiving feedback on those referrals creates a wealth of data. That data can be used to understand better populations, the community, and gaps in where and how policy can be influenced to make needed structural changes that precipitate recurring cycles of social needs. Below are tools and resources to assist in that analysis.
Unite Us can combine large consumer and health care data sets to better understand risk factors and provide guidance for policy and decision making. (Website)
 Socially Determined
Socially DeterminedSocially Determined describes population-level analytic solutions as paths to surfacing SDOH insights to help organizations understand social risk dynamics and create actionable programs. (Website)
 The Gravity Project
The Gravity ProjectEstablished by the Social Interventions Research & Evaluation Network (SIREN), the Gravity Project works to identify and harmonize social risk factor data for interoperable electronic health information exchange. (Website)
 Health-Related Quality of Life (HRQOL)
Health-Related Quality of Life (HRQOL)
“Healthy Days Measures” are a set of questions developed by the Centers for Disease Control & Prevention (CDC) to estimate the number of recent days when a person’s physical and mental health was good (or better). They can serve as a proxy for measuring return on investment. (Website)
 Shared Principles for Measuring SDOH Interventions
Shared Principles for Measuring SDOH Interventions
A call-to-action paper from The National Alliance to Impact the Social Determinants of Health (NASDOH) intended to motivate conversation and action around measuring the success of SDOH interventions. (6-page PDF)
 Evaluation Measures for SDOH Programs
Evaluation Measures for SDOH Programs
The Rural Health Information Hub (RHIhub) offers tools and techniques to enable short-term and intermediate SDOH outcome measures and process measures. Additional information on identifying strategies and measures for gathering appropriate data and evidence can be found in their Rural Community Health Toolkit. (Website)
SDOH and Rural Health
Rural America experiences many inequities compared to the nation as a whole. Often rural residents have fewer individual resources and, on average, are poorer and less educated. Additionally, many rural minorities face discrimination and racism that can result in stress, negatively impacting their health. Unfair treatment may impact rural minorities’ ability to fully access services to support health, including health care services. Below are tools and resources to address SDOH in rural areas.
 Understanding and Addressing Social Determinants of Health: Opportunities to Improve Health Outcomes
Understanding and Addressing Social Determinants of Health: Opportunities to Improve Health Outcomes
This guide provides rural health care leaders and teams with foundational knowledge, strategies, and resources to understand the impact of social determinants of health (SDOH) on patients and communities. It organizes key information and resources to help the busy manager support and lead education and discussion with front-line staff. (11-page PDF)
![]() Social Determinants of Health for Rural People
Social Determinants of Health for Rural People
This guide describes how income level, educational attainment, race, and where you reside impact health. The guide includes statistics and frequently asked questions on the health inequities that rural residents experience. (Website)
Actions to Address SDOH
Review and follow up on these actions to address social determinants of health—to enhance those factors that result in positive outcomes and remedy those factors that result in adverse or disparate outcomes.
Learn more about SDOH and how they influence the health of patients in positive and negative ways:
- Healthy People 2030 offers basic information about SDOH.
- County Health Rankings Model explores and quantifies factors influencing how long and how well we live. Explore this model to understand better the social factors that influence health.
Suggested questions for team discussion:
- What surprised you about factors influencing how long and well we live?
- What SDOH affect people in our community (e.g., access to healthy food, unsafe housing, reliable transportation), and how do those impact health?
- How might taking action to improve the conditions in people’s environment improve health locally?
- What processes does our organization have to help individuals address SDOH—their social needs?
County Health Rankings & Roadmaps provides information on the health of your county and factors that drive its ranking. Scroll down to the “How Healthy is Your Community” section and enter your state, county, or ZIP code to review health outcomes, health factor data, and rankings. Then, select “areas to explore,” and specific findings will be highlighted.
Suggested questions for team discussion:
- Which of these “areas to explore” significantly influence health in our community or county?
- What social conditions might contribute to these factors (for example, poverty or living in a rural setting)?
After your team has reviewed data (County Health Rankings & Roadmaps) on health disparities, demographics, health care access, SDOH, and more, identify opportunities for action.
Suggested questions for team discussion:
- What are key SDOH impacting our patients and community members?
- How are these SDOH impacting health and health outcomes?
- What strategies have already been implemented, and what has worked well in addressing SDOH that negatively impacts health in our health care system and our community (for example, initiatives to increase access to fruits and vegetables or physical activity)?
- What are additional priority areas we could work on to address SDOH that are negatively impacting health?
- Are there opportunities to better connect patients and families to current initiatives that help address social needs in our organization, health care system, and community?
- What can we learn from other organizations, healthcare systems, communities, and healthcare professionals in how they address SDOH? What ideas are inspiring? What initiatives might we consider in our organization and community? For example, review community stories about other communities and providers addressing SDOH (filter stories by state, partners, health factors, and more.)
- What community partners should we work with to leverage resources to address SDOH (social needs of our community)?
- What barriers have we faced in addressing SDOH in our organization and community? How have we or can we overcome these barriers?
- What is the clinician’s role in population health and supporting the integration of SDOH into health care?
- Social Determinants of Health 101 for Health Care: Five Plus Five describes five things we know about SDOH and five things we need to learn to address SDOH. The article discusses several concerns that clinicians may raise about involvement in SDOH.
In working through the SDOH information on Culture Care Connection, you and your team have built foundational knowledge to understand the impact of SDOH on your patients and community and the need and opportunity to address these factors that negatively impact health. You have reviewed data to support decision-making and are ready to synthesize the information and plan, implement, and measure steps to address SDOH.
Suggested questions for team discussion:
- How can we get involved in or lead efforts in our community to address SDOH that negatively impact the health of our health system and community members?
- What processes can our organization put in place to support individual patients and families
with SDOH needs? - How will we prioritize where to focus, and what will we work on first?
- What do we need to do to get started?
- What resources can we draw on to support our efforts to address SDOH?
- What measures can we use to evaluate our work and its impact?
Review Take Action to Improve Health (County Health Rankings & Road Maps Action Center) to help you develop a plan and find strategies that we know work, guidance for setting a plan in motion, and resources to help you partner with others.
In this resource:
- Go to Action Center to review five steps to address SDOH that negatively impact health, and improve health equity:
- Assess needs and resources
- Focus on what is important
- Choose effective policies and programs
- Act on what is important
- Evaluate actions
- Go to What Works for Health to find strategies by topic. The best available evidence is summarized, and policies and programs that can help improve health behaviors, clinical care, social and economic factors, and the physical environment are shared. Strategies can be sorted by “decision-makers,” such as health care, public health, or nonprofits, to generate ideas for where your organization might lead efforts to address SDOH.